 Boris Johnson Was Secretly ‘Nudged’ into Wearing a Mask by SAGE Scientists
Boris Johnson Was Secretly ‘Nudged’ into Wearing a Mask by SAGE Scientists National Census: Only 0.2% of the Population Define Themselves as ‘Trans’
National Census: Only 0.2% of the Population Define Themselves as ‘Trans’
Are All the Heart Attacks Really Due to a Lack of Statins?
On December 1st, the U.K. Government published a technical report on the Covid pandemic.

We commented on it in our post and its late pick-up by the mainstream media and their lack of critical approach to its ‘independent’ content.
One of the paragraphs that interested us is the one in which the Chief Medical Officer explained the non-Covid related excess mortality most European nations are experiencing:
There is little doubt that delays in presentation, reductions in secondary prevention (such as statins and antihypertensives) and postponement of elective and semi-elective care and screening will have led to later and more severe presentation of non-Covid illness both during and after the first three waves. The combined effect of this will likely lead to a prolonged period of non-Covid excess mortality and morbidity after the worst period of the pandemic is over.
There can be little doubt that blocking access to, say, cancer screening and treatment will have disastrous consequences – one of the many legacies of lockdowns. But how did Professor Whitty and his team conclude that excess cardiovascular mortality was due to a lack of statins and antihypertensives?
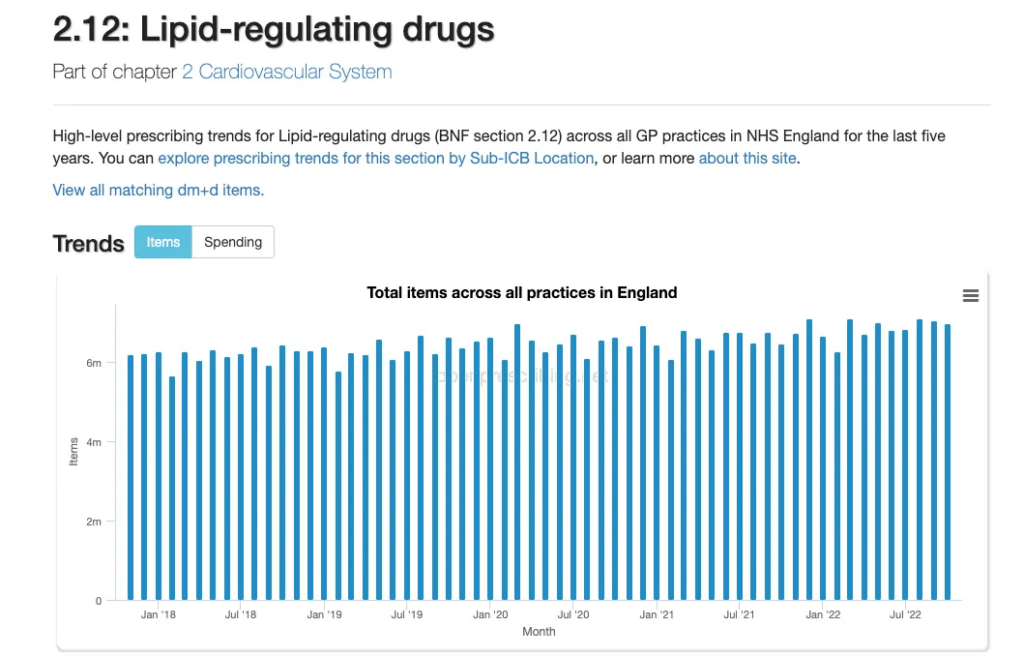
Primary care is where the bulk of statins and antihypertensives are prescribed, but did the prescriptions of such drugs change during the pandemic?
Not according to Open Prescribing, which is based on monthly NHS prescribing data.
Another aspect that needs to be considered when looking at whether a lack of statins could have caused a sudden increase in cardiovascular deaths is the length of time of exposure to the drugs.
A large meta-analysis of the effects of statin use in primary prevention compared to placebo reported a number-needed-to-treat (NNT) of 138 people with statins for five years to prevent one death, 49 to prevent one cardiovascular disease (CVD) event, and 155 to prevent one stroke.
The figures for secondary prevention (in those who have known heart disease or a history of stroke) are better, as you would expect: NNT of 83 for one death after five years of exposure to a statin.
The five years do not fit the introduction of restrictions in March 2020, nor is there any evidence that lipid regulating and antihypertensive drugs were prescribed less in the last three years based on the NHS’s data.
There is evidence of a fundamental change in working practice and primary care delivery during the three periods of restrictions. Six measures recovered to pre-pandemic levels within a year, asthma and COPD (pulmonary disease) reviews recovered by August 2021, and blood pressure monitoring and cardiovascular disease risk assessment had a sustained drop in activity up to December 2021.
However, a sustained drop in monitoring is unlikely to be the reason for the increase in excess deaths. In 2017 we did a systematic review of the effect of global cardiovascular risk assessment in adults. We found its use did not translate into reductions in CVD morbidity or mortality.
So what might be the cause? The British Heart Foundation considers “severe ambulance delays, inaccessible care and ever-growing waiting lists are contributing to heart patients dying needlessly”.
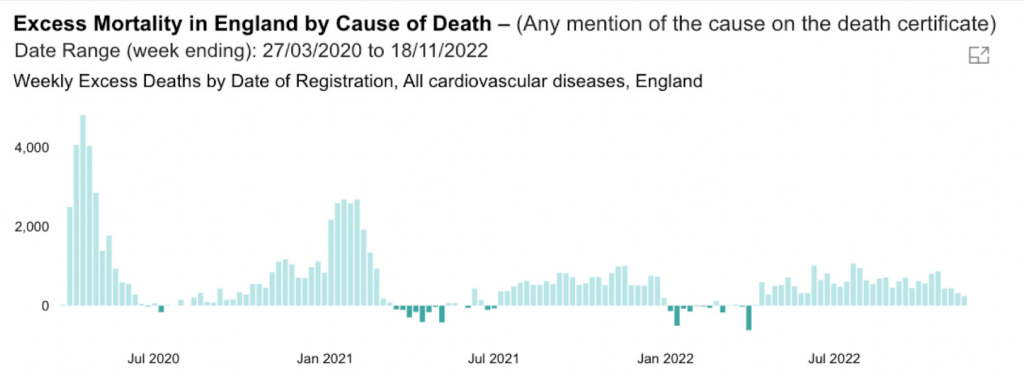
While the data from the Office for Health Improvement and Disparities report an excess of cardiovascular disease mortality, the ‘independent’ report produced by the U.K. Government does not attempt to understand what is causing the excess mortality from CVD.
In the last year, there has been an excess of 21,841 deaths with CVD mentioned on the death certificate. Our analysis suggests it isn’t a fall in drug treatment, and the drop in CVD risk monitoring can’t account for it, given the lack of evidence of an effect.
Given all its resources, the Government could and should do better to get to the bottom of what is driving the excess in cardiovascular deaths. We’ll keep digging.
Dr. Carl Heneghan is the Oxford Professor of Evidence Based Medicine and Dr. Tom Jefferson is an epidemiologist based in Rome who works with Professor Heneghan on the Cochrane Collaboration. This article was first published on their Substack blog, Trust The Evidence, which you can subscribe to here.







