
Secrets of the Pandemic

Published: July 2022
Share on: TW / FB / TG
Little-known aspects of the coronavirus pandemic.
Contents
Pandemic Response: Failure or Success? / The SARS&MERS “Death Rate” / China & Zero Covid / Coronavirus Origins / Why Face Masks Have Failed / The Dark Side of Covid Vaccine Trials / Covid Treatment: Antivirals & More / Asymptomatic Transmission / Long Covid / Children
Pandemic Response: Failure or Success?
The international pandemic response has generally been perceived as a total disaster and a complete chaos. Yet this is only true if seen from a public health perspective. If seen from a technological and strategic perspective, the response may be described as an unprecedented success.
Within months of the WHO pandemic declaration in March 2020, PCR genetic tests became widely available, Apple and Google inserted contact tracing interfaces into the operating systems of billions of mobile phones, and numerous governments had developed contact tracing apps. Within less than a year, novel “programmable” mRNA vaccines became available internationally. And in March 2021, Israel was the first country to introduce a digital vaccination certificate (“Green Pass”), followed by almost every other country in the world, including no-lockdown Sweden. Throughout this time, digital technologies were leveraged to manage remote work, remote learning and lockdowns, enforced in some places by the use of modern police drones and robotic dogs.
None of these innovations worked to contain or stop the pandemic, and none of them had been recommended by existing pandemic guidelines. Yet most of these policies were recommended by billionaire-funded organizations such as CEPI and GAVI, and many of them were publicly announced in March 2020 by the “world’s most powerful doctor” (Politico), Bill Gates, a major sponsor of the World Health Organization and a leading investor in mRNA vaccine technology.
Furthermore, most of these innovations tie in neatly with other strategic initiatives, such as the WEF-linked ID2020 digital identity program, or they might be repurposed later on in the context of “climate change policy”, “terrorism prevention”, or Chinese-style “social credit” population control systems. In this regard, Israeli military historian and “WEF philosopher”, Yuval Harari, argued already in October 2020 that “Covid is critical, because this is what convinces people to accept, to legitimize total biometric surveillance.”
It is also noteworthy that while lockdowns, face masks and covid vaccines totally failed to stop coronavirus transmission, the false idea that they could stop transmission was crucial to justifying the introduction of QR-based digital vaccination certificates in the first place. The EU recently decided to extend the legal basis of these certificates for another year, while the US is about to fire 60,000 unvaccinated National Guard and reserve soldiers.
Read more: Did CEPI’s bio-spooks lock down the West? (TCW) and Cock-up or Conspiracy? Understanding COVID-19 as a ‘Structural Deep Event’ (Dr. Piers Robinson)
The Dubious SARS/MERS “Death Rate”
A quite important yet mostly overlooked aspect of covid fearmongering was the comparison of SARS-CoV-2 to SARS and MERS. Specifically, the media and many scientists repeatedly stated that SARS had a “death rate” of 10% and MERS had a “death rate” of 35%, which made it seemingly reasonable to assume that SARS-CoV-2, a SARS-like coronavirus, might also have a “death rate” of at least several percent and might kill hundreds of millions of people, or even a third of mankind.
Yet a quick review of these “death rates” shows that these are not, of course, infection fatality rates, but case fatality rates, and the “cases” were not just any cases, but mostly patients hospitalized with a severe case of SARS or MERS. This is because during both the SARS outbreak in 2002-2003 and the MERS outbreak in 2012-2015, there was not yet any PCR mass testing available, and only severe cases were tested at all.
Thus, it is quite likely that the original SARS and MERS outbreaks were in fact larger than recorded, and the SARS and MERS infection fatality rates in the general population were much lower, perhaps only a fraction of one percent, similar to the infection fatality rate of SARS-CoV-2.
Ironically, if the recent pandemic had been caused by an aggressive influenza virus instead of a coronavirus, the actual death rate, especially in young people, could have been much higher.
See also: Covid fatality rates (SPR)
China and Zero Covid
China is the last country on Earth to still pursue a hopeless “zero covid” policy, and Chinese authorities continue to impose devastating lockdowns on major cities such as Shanghai and Beijing. Various theories have been proposed as to why China would follow such a seemingly irrational and destructive policy, including “China is deceiving the West”, “China is putting health over profits”, or “China deliberately disrupts Western supply chains”.
Yet most likely, the Chinese government simply doesn’t want to admit defeat against coronavirus. Furthermore, the fact that the US suffered one million covid deaths and India suffered three to five million covid deaths, while China until 2022 had suffered very few covid deaths, is seen as confirmation that China is in fact a superior civilization.
The Chinese government is also perhaps the most technocratic government in the world, and they are the only government that has even tried to preempt or disrupt aerosol transmission, which comes at an enormous economic and social cost. Finally, the Chinese government likely sees covid as an opportunity to further enhance its QR-based population control scheme.
Remarkably, though, Beijing city authorities recently had to withdraw a planned vaccination mandate for some public venues after massive online protest by citizens.
To get a glimpse of the Chinese “zero covid” reality, see the eye-opening Twitter video channel of “Songpinganq” (16+, contains disturbing footage). To learn more about the Chinese digital “social credit” system, see this 5-minute report by France24.
See also: Did China stage the early covid videos? (SPR)
Coronavirus Origins
As previously discussed, the novel coronavirus almost certainly emerged out of US-Chinese virological research. Moreover, the current omicron variant, which features two dozen immune-evasive spike mutations “copied from scientific publications”, most likely emerged from pan-coronavirus vaccine research (presumably in a South African lab).
Thus, within the span of just three years, the world has likely seen not one, but two man-made virus pandemics. After the delta variant, several countries with covid infection rates above 70% had achieved a kind of “herd immunity” and had seen the return of influenza viruses (e.g. India, Brazil and Sweden); yet the immune-evasive (but milder) omicron variant has undone this achievement and has launched several massive new waves within just a few months.
Most recently, the Chair of the Lancet Covid Commission, US professor Jeffrey Sachs, stated that he is “pretty convinced [SARS-CoV-2] came out of US lab biotechnology, not out of nature” and that this is “not being investigated, not in the United States and not anywhere, for real reasons… I believe they do not want to look under the rug too much.” Professor Sachs also wrote an in-depth article and a scientific paper on the likely origins of SARS-CoV-2.
A lab-related virus origin either in China or in the US, and either accidental or deliberate – all of these possibilities remain entirely plausible. In particular, a deliberate release does not even have to be a “conspiracy”, as any single researcher involved in this type of research could decide to release such a pathogen, as the US FBI (falsely) claimed in the case of the 2001 anthrax letters.
See also: On the Origins of SARS-CoV-2 (SPR)
Why Face Masks Have Failed
It has been known for decades that face masks don’t work against respiratory virus epidemics, and the current coronavirus pandemic has once again confirmed this reality. Even N95/FFP2 masks have had no impact on infection rates in the general population, neither in Germany and Austria, nor in Taiwan and South Korea (which saw record infection rates in recent months).
A recent Australian study, published in the Journal of Infectious Diseases, has finally shown why face masks fail so badly. The experimental study for the first time used actual virus aerosols (of a virus harmless to humans) and actual humans (not puppet heads) in an aerosol chamber.
The study found that neither face masks nor unfitted N95/FFP2 masks had any measurable effect on virus loads in the nostrils of study participants; only fit-tested N95/FFP2 masks significantly and strongly reduced virus loads in nostrils, as they prevent aerosols from bypassing the mask.
This result is fully consistent with real-world observations that face masks and N95/FFP2 masks worn by the general population are useless, whereas fit-tested N95/FFP2 masks worn by medical professionals can make a real difference – although during an epidemic, medical professionals may then get infected at home or during social activities, as masks cannot be worn 24/7.
See also: The Face Mask Folly in Retrospect (SPR)
The Dark Side of Covid Vaccine Trials
How sincere were the original covid vaccine trials?
It was already known that the Russian Sputnik vaccine trial most likely forged its results (to achieve an efficacy at least as high as Western mRNA vaccines). It was also known that both AstraZeneca and Johnson&Johnson declared some severe adverse events that were likely related to the vaccine – a case of transverse myelitis and a case of cerebral sinus venous thrombosis – as being “unrelated”.
Furthermore, it was known that the Pfizer vaccine trial had strangely excluded, without explanation, five times more people from the vaccine group than from the control group.
Pfizer and the US FDA attempted to hide the original Pfizer vaccine trial documents for a full 75 years, but a determined New York lawyer forced them to immediately release the documents on a monthly basis. While almost totally ignored by traditional media, many of these documents have already been analyzed by independent investigators who coordinate themselves on Twitter.
Their preliminary results indicate that Pfizer and its subcontractors (which ran the trial sites) really may have suppressed some serious vaccine adverse events (by excluding the participants or by miscategorizing the events) and may have exaggerated vaccine efficacy (by not testing symptomatic participants or by simply excluding positive participants).
There have also been claims that hidden anti-N antibody data showed that the Pfizer vaccine actually had zero efficacy, but this was not the case: most of these infections occurred prior to the second vaccine dose or shortly thereafter.
To learn more about the dark side of the Pfizer vaccine trial, take a look at the following articles:
- Deaths After Vaccination in Pfizer Trial Not Fully Investigated, New Documents Reveal (Daily Sceptic)
- Pfizer Classified Almost All Severe Adverse Events During COVID Vaccine Trials ‘Not Related to Shots’ (CHD)
- Is Subject #12312982 the Key to Proving Pfizer Vaccine Trial Fraud? The Story of Augusto Roux (Josh Guetzkow)
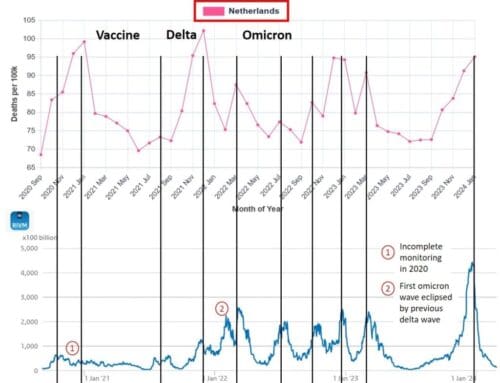
The covid vaccines may have saved a few million lives in 2021, mainly by mitigating the alpha and delta waves in Europe, the United States and elsewhere (though not “20 million lives” as recently claimed by some Gates-funded researchers). But vaccine protection even against severe disease is rapidly waning: the Netherlands recently reported 77% protection after four doses weeks ago, 63% protection after three doses months ago, and 0% protection after two doses a year ago.
Overall, covid vaccines may yet win a Nobel Prize in Medicine, or turn out to be the biggest medical scandal in recent history, or perhaps both. At any rate, the vaccination of people not at risk of severe acute covid was almost certainly a mistake, and in some cases a crime.
See also: Covid Vaccine Adverse Events (SPR)
Covid Drugs I: The Failure of Antivirals
To treat covid, pharmaceutical companies mostly focused on the development of novel and rather expensive antiviral drugs. Yet all of these drugs, sold for billions of dollars to desperate health authorities, ultimately failed.
Antiviral drugs that were given only to hospitalized patients with severe covid had to fail almost by definition, as most of these patients had already progressed to the post-viral, hyper-inflammatory phase of covid. This was the case of convalescent plasma therapy and Gilead’s highly expensive yet toxic and totally ineffective Remdesivir.
Monoclonal antibodies, which were given to high-risk outpatients as quickly as possible, initially proved effective, but they lost the battle against new coronavirus mutations.
Merck’s Molnupiravir was a non-starter, both ineffective against most variants and dangerously mutagenic (“avoid unprotected sex for 30 days after treatment”).
Pfizer’s Paxlovid, which directly inhibits the main coronavirus replication enzyme, looked most promising. Yet it soon turned out that it was effective only in unvaccinated high-risk patients, not in standard-risk patients or in vaccinated high-risk patients. Moreover, up to half of all patients experienced a “covid rebound” immediately after discontinuing the drug; the side effect profile was worse than expected (“Paxlovid mouth”); and SARS-CoV-2 quickly started developing Paxlovid-resistant mutations. Another expensive bummer.
SPR had warned in advance that Remdesivir was a fraud, Molnupiravir was outright dangerous, and Paxlovid might lead to rapid reinfections. The reality is that antiviral drugs may simply not be the ideal choice against a ubiquitous and fast-mutating respiratory virus.
Covid Drugs II: Ivermectin, HCQ, and more
Given the many issues with antiviral drugs, another approach to tackle covid is to try to improve the immune response and to mitigate the health impact of the virus.
At the population level, this could be done by reducing obesity rates, since obesity has been shown to be linked to an ineffective and even destructive immune response. It could also be done by removing any deficiencies in vitamins and minerals (e.g. vitamin D and zinc).
Two of the most controversial covid treatments during the pandemic have been Nobel Prize-winning anti-parasitic drug ivermectin and history-making anti-malaria drug HCQ. Most trials of these and other off-patent drugs were rather pointless, involving low-risk participants, late administration, or unrealistic endpoints (e.g. infections or symptom duration instead of disease progression).
Nevertheless, concerning ivermectin, a yet unpublished, updated meta-analysis of non-fraudulent trials indicates that ivermectin is indeed about 30% effective at reducing severe and fatal covid. Furthermore, the lead investigator of the TOGETHER trial acknowledged in a leaked email that “there is a clear signal that ivermectin works in COVID patients”. The renowned French Institute Pasteur previously found a “more favorable clinical presentation” in a detailed coronavirus animal study.
The apparent usefulness of ivermectin is most likely not due to an anti-viral effect, but due to the known immuno-modulatory and anti-asthma effects. This would also explain why Merck, in early 2021, claimed ivermectin was “not effective”: if anything, they only looked into anti-viral activity.
Concerning HCQ, an updated retrospective study from the group of French professor Didier Raoult found a 30% effectiveness against death in hospitalized patients, and a similar or higher effectiveness in outpatients. A yet-to-be-published meta-analysis also found a 30% effectiveness against hospitalization and death in high-risk outpatients.
In the case of HCQ, the apparent usefulness is most likely not due to an anti-viral effect, either, but instead due to the known anti-coagulation and anti-autoimmune effects.
In sum, it looks like some of these medications could really have been beneficial in reducing the risk of severe covid, but they clearly did not “crush the curve” anywhere.
See also: On the treatment of covid (SPR)
Asymptomatic Transmission: A Myth?
Many authorities tried to use the idea of “asymptomatic transmission” to justify mask mandates and lockdowns, while many skeptics pushed back by arguing that “asymptomatic transmission” was a myth. In truth, asymptomatic and especially pre-symptomatic transmission are real and well-known from influenza and other viruses, but due to aerosol transmission, face masks and other restrictions still don’t work.
Some recent press reports claimed that a new meta-study showed “asymptomatic transmission” was very rare, but the meta-study in fact showed the opposite: it found that pre-symptomatic transmission was just as likely as symptomatic transmission (risk ratio 1.00) and that it accounted for 30% to 50% of all transmission. Only people that remain fully asymptomatic throughout their infection are less likely to infect others (risk ratio 0.32), likely because of a lower viral load.
Indeed, without insidious pre-symptomatic aerosol transmission – which doesn’t require any “droplets” produced by coughing or sneezing – the coronavirus pandemic would probably not have been possible. Given that aerosol transmission occurs almost only indoors and face masks are ineffective against aerosols, public health policy should likely focus on improving indoor air quality, especially in important public venues.
See also: Pre-symptomatic transmission is very real (SPR)
Long Covid: Another Myth?
Similar to the case of “asymptomatic transmission”, many health authorities tried to use the risk of “long covid” to justify mask mandates or vaccination mandates even for young people, while many skeptics tried to push back by arguing that “long covid” was a myth or a psychological condition.
Yet ever since the summer of 2020, the clinical reality of long covid has been obvious, and it has also been clear that long covid can seriously impact the quality of life and performance even of previously healthy young people who had only seemingly mild covid.
The pathology of long covid isn’t a total mystery anymore, either. First, there are patients who do not (fully) recover their sense of taste or smell. Second, there are patients who show respiratory problems due to asthma-like conditions, gas exchange abnormalities, or lung perfusion (blood flow) issues (likely due to endothelial damage). Third, there are patients who develop new-onset neurological or auto-immune conditions that are often difficult to diagnose.
On the other hand, heart inflammation is not generally a covid or long covid risk, but rather a covid vaccination risk, especially in young males.
Studies that claim “long covid” is a myth typically make one of three mistakes: first, they compare non-specific symptoms unrelated to covid and long covid; second, they rely on unreliable antibody data; or third, they assume that if a general practitioner cannot identify a cause, no cause exists.
In this regard, a study recently published in Lancet eBioMedicine found that almost 50% of long covid patients that showed no SARS-CoV-2 antibodies did show a SARS-CoV-2-specific T-cell response (i.e. they had been infected). It is also known that some widely used antibody tests (e.g. Abbott) have a sensitivity of just 20% one year after mild infection.
The real questions concerning long covid are rather these: how many people are affected, how severe are these cases, what is the recovery rate, do reinfections increase the risk of long covid or exacerbate long covid, and are there any treatments?
For instance, a recent German insurance study found that among covid patients in 2020, 1% to 5% received a medical long covid diagnosis in 2021; the average long covid sick leave from work in 2021 was 90 days even in non-hospitalized patients, and 105 days overall.
Denying long covid is about as reasonable as denying vaccine injuries. It is part of the complex reality of this pandemic, unfortunately, even though the condition has indeed sometimes been abused for fearmongering and political ends.
Read more: Post-Acute Covid and Long Covid (SPR)
Children: From Little Heroes to Big Losers
A comprehensive Icelandic study recently confirmed once more that covid remained asymptomatic or mild in almost all children, and that prior to omicron, almost 90% of infections in children occurred outside of school, mostly at home, and mostly from adults to children, not the other way around (omicron removed this difference to some extent).
On the other hand, UNESCO found that over 150 million children missed more than half a year of in-person schooling (and up to two years in some countries), which caused reading and math abilities to decline substantially, especially in developing countries. According to the World Bank, the pandemic response has caused “the worst educational crisis for a century, and certainly since the world wars.”
Children should have been the little invincible heroes of this pandemic, but unfortunately in many countries they have been turned into perhaps the biggest losers. If there is one lesson to be learned from this pandemic, it is to never repeat this mistake.
See also: Covid and Kids: The Evidence. (SPR)
You have been reading: Secrets of the Pandemic.
An analysis by Swiss Policy Research.
Read more
Share on: Twitter / Facebook / Telegram



![[German] Die RAF-Täuschung](https://b2400116.smushcdn.com/2400116/wp-content/uploads/2024/03/1191051-german-die-raf-taeuschung-500x383.webp?lossy=2&strip=1&webp=1)
![[German] Das Phantom der RAF](https://b2400116.smushcdn.com/2400116/wp-content/uploads/2024/03/1194227-german-das-phantom-der-raf-500x383.webp?lossy=2&strip=1&webp=1)